前文
レビー小体型認知症(dementia with Lewy bodies; DLB)は,アルツハイマー病(Alzheimer’s disease; AD)の次に多い変性性認知症である.DLBは認知機能低下に加え,幻視,うつ症状,嫉妬妄想などの精神症状,抗精神病薬に対する過敏性,認知機能の変動(fluctuation),パーキンソニズム,注意機能の低下,遂行機能障害,レム期睡眠行動異常症(rapid
eye movement sleep behavior disorder; RBD)などの症状が見られる1).ADと比べDLBは比較的記憶機能が保たれている一方,遂行機能障害と視空間認知障害が特徴とされ,早期より視覚構成機能の低下があり,幻視や誤認との関連が示唆されている.DLB症候に関連した画像所見として脳血流Single
Photon Emission Computed Tomography(SPECT)では後頭葉の血流低下が知られている.1997年に馬蹄型の後頭葉の血流低下が報告され2),その後,幻視を伴うDLB患者の57.7%に後頭葉血流低下が見られたとの報告もされた3).Positron Emission Tomography(FDG-PET)の研究でも2008年幻視のある患者で右後頭-側頭結合部と左中前頭回で代謝低下が報告され4),2010年に人の幻視や実体意識性の幻覚は,脳SPECTの左腹側後頭葉の血流低下に関連するとの報告があった5).以上からDLB患者に見られる後頭葉の代謝あるいは血流低下と,幻視あるいは神経心理学的症候との関連が強く示唆されている.
2017年に改訂されたDLBの診断基準では核医学検査の重要性が強調され,指標的バイオマーカーには,大脳基底核でのドパミントランスポーター取り込み低下,123I-metaiodobenzylguanidine(MIBG)心筋シンチグラフィーで取り込み低下などが含まれ,支持的バイオマーカーには,脳血流SPECT/PETで後頭葉にめだつ取り込み低下,フルオロデオキシグルコースを用いたFDG-PETでの帯状回島兆候(cingulate
island sign; CIS)が含まれた1).
DLB患者のFDG-PETにおけるCISは,周囲の糖代謝低下と比較して,後部帯状回から楔前部・楔部の循環・代謝が比較的保たれている特徴的所見であり,ADでは後部帯状回の糖代謝が早期より低下することから,ADとDLBの鑑別に役立つとされている.この所見は,脳血流SPECT画像でも検討されてきた.CIScoreはeZISニューロVer-1.1.0.0(冨士フィルム富山化学株式会社)上で自動的に算出されるスコアで,後頭葉を中心とするDLBの疾患特異領域(Region
of interest 1; ROI-1)とADの疾患特異領域からDLBの疾患特異領域を除いた後部帯状回を中心とする領域(ROI-2)の二つのROIが自動的に設定され,ROI-2における血流低下側のZスコア合計をROI-1における血流低下側のZスコア合計で除することによりCIScoreが算出され,CIScore
0.281未満がDLBの可能性が高いと報告されている6).また,DLB診断において感度92.3%,特異度76.9%,正診率84.6%との報告がある6)7).
一方神経心理学的評価法としてAlaらは,DLBの特徴である記憶,注意,視覚構成機能の障害に関連するMMSE(Mini-Mental State Examination)の下位項目(注意:Serial7,記憶:遅延再生,構成:図形)を用いて,「Ala
Score=注意-5/3×記憶+5×構成」の公式を提唱し,Ala Scoreが5点未満であれば,ADよりもDLBである確率が高いとした8).
Ala ScoreとCIScoreはともにDLBを鑑別するために開発されたものであるが,この両者の関連を比較した研究はこれまでにない.CISは2017年のDLB診断基準に含まれているものの,支持的バイオマーカーの位置づけとなっており実際の診断には影響しない.しかしこれまでの研究ではCIScoreの感度,特異度は比較的高く,実際の臨床での有効性が期待される.両方実施できる施設での感度,特異度の向上について,また一般クリニックには必ずしもSPECTの機械設備があるとは限らず,Ala
Scoreが検査の代替評価となるかどうか検討するため,今回,両者の関連および,ADとDLBの鑑別においての有用性について検討した.
方法
2011年1月~2018年5月に当院脳神経内科,物忘れ外来を受診した患者でMMSE,99m Tc-ECD SPECTを実施した連続症例77名(2017年の診断基準1)にのっとって,最終診断としてDLB 35名:probable DLB 32名,possible DLB 3名,2011年のNIA-AAによるガイドライン9)にのっとった診断としてprobable AD 42名)のAla ScoreとCIScore,MMSE下位項目とCIScoreについて相関分析を行った.
撮像機器は,2014年4月10日までの検査はPRIZM 3000 IRIX(Philips社製),3検出器型,それ以降の検査はGCA-9300R(キャノンメディカルシステムズ社製),3検出器型の2機種を使用した.PRIZM
3000 IRIX,3検出器型,低エネルギー高分解能型コリメータ(LEHR)を用いて,収集条件は99m Tc-ECD 600 MBq投与後5分から16分間データ収集(4度/Step,
90 view),マトリクスは128 × 128,画像再構成はFiltered back projection(FBP)法で行った.GCA-9300R,3検出器型,高分解能型ファンビームコリメータ(FAN HR)を用いて,収集条件は99m Tc-ECD 600 MBq投与後5分から16分間データ収集(4度/Step, 90 view),マトリクスは128 × 128,画像再構成はThree-dimensional ordered subset expectation maximization method(3D-OSEM法)で行った.2機種とも前処理フィルタはButterworth filter,減弱補正はChang,散乱補正はTriple energy
window(TEW)法で行った.なお,Hoffmanファントムを用いて機種間補正を行っている.
(1)まず,79歳以下の群39名(DLB 20名,AD 19名),80歳以上の群38名(DLB 15名,AD 23名)と年齢のみで群分けし,Ala ScoreとCIScoreについてはPearsonの積率相関係数を算出し,MMSE下位項目とCIScoreについてはSpearmanの順位相関係数を算出した.
(2)次に年齢群に加え,疾患別の群に分けて相関分析を行った.79歳以下DLB群20名,79歳以下AD群19名,80歳以上DLB群15名,80歳以上AD群23名の4群に群分けし(Table
1),Ala ScoreとCIScore,MMSE下位項目とCIScoreについて相関分析を行った.(1),(2)の統計ソフトはIBM SPSS Statisticsバージョン24を使用した.
Table 1
The mean value of each score, correlation coefficient between CIScore and Ala Score,
and MMSE subscore.
|
|
≦79 yrs.
AD+DLB
(n = 39)
|
≧80 yrs.
AD+DLB
(n = 38)
|
≦79 yrs.
AD
(n = 19)
|
≦79 yrs.
DLB
(n = 20)
|
≧80 yrs.
AD
(n = 23)
|
≧80 yrs.
DLB
(n = 15)
|
|
Total number
|
39
|
38
|
19
|
20
|
23
|
15
|
|
Male
|
17
|
11
|
6
|
11
|
5
|
6
|
|
Female
|
22
|
27
|
13
|
9
|
18
|
9
|
|
Average age
|
73.15 ± 4.73
|
82.76 ± 2.31
|
71.53 ± 5.07
|
74.70 ± 3.90
|
82.78 ± 2.37
|
82.73 ± 2.28
|
|
Average MMSE
|
22.33 ± 3.79
|
20.74 ± 3.83
|
22.00 ± 4.28
|
22.65 ± 3.35
|
20.61 ± 3.26
|
20.93 ± 4.70
|
|
Average Ala Score
|
4.32 ± 2.94
|
4.23 ± 2.98
|
5.88 ± 2.36
|
2.85 ± 2.69
|
5.71 ± 2.14
|
1.96 ± 2.67
|
|
Average CIScore
|
0.30 ± 0.19
|
0.45 ± 0.33
|
0.42 ± 0.20
|
0.19 ± 0.07
|
0.56 ± 0.36
|
0.29 ± 0.18
|
|
Correlation with CIScore (Pearson) |
|
Ala Score
|
0.485**
|
0.285
|
0.481*
|
–0.241
|
0.148
|
–0.214
|
|
P value
|
0.002
|
0.083
|
0.037
|
0.306
|
0.500
|
0.443
|
|
MMSE total
|
–0.042
|
–0.193
|
0.099
|
–0.283
|
–0.305
|
–0.026
|
|
P value
|
0.802
|
0.246
|
0.685
|
0.226
|
0.158
|
0.928
|
|
Correlation with CIScore (Spearman) |
|
Orientation (Time)
|
–0.447**
|
–0.412*
|
–0.226
|
–0.470*
|
–0.347
|
–0.304
|
|
P value
|
0.004
|
0.010
|
0.352
|
0.036
|
0.105
|
0.271
|
|
Calculation
|
0.204
|
0.282
|
0.282
|
–0.230
|
0.179
|
–0.099
|
|
P value
|
0.212
|
0.086
|
0.241
|
0.328
|
0.414
|
0.725
|
|
Recall
|
–0.264
|
–0.366*
|
–0.241
|
–0.024
|
–0.378
|
–0.126
|
|
P value
|
0.104
|
0.024
|
0.320
|
0.921
|
0.075
|
0.654
|
|
Order
|
–0.273
|
0.158
|
–0.165
|
–0.427
|
0.089
|
0.351
|
|
P value
|
0.093
|
0.342
|
0.499
|
0.060
|
0.686
|
0.200
|
(3)各群の感度,特異度を算出し,ROC曲線の曲線下面積(area under the curve; AUC)の比較を行った.統計ソフトはEZR on R commander10)version 1.35を使用した.
本研究は,福岡大学医学部の倫理委員会で承認済みである.承認番号:2018M036,承認日:2018年7月5日
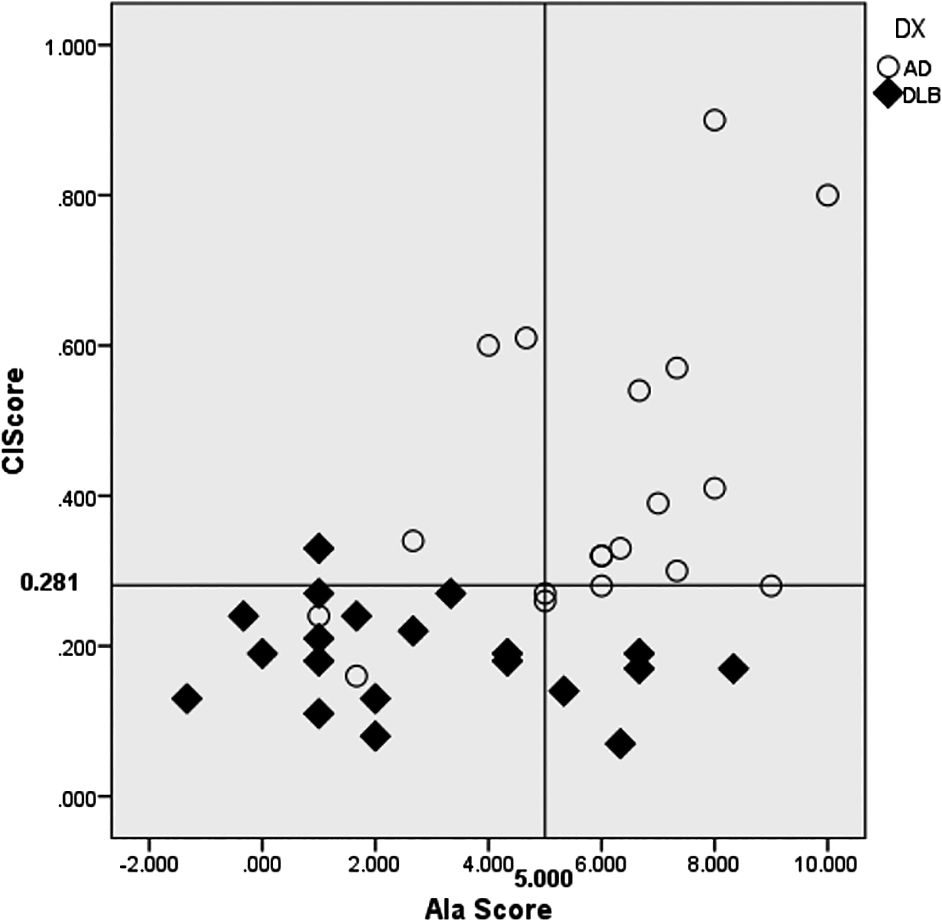
Fig. 1
Scatter plot image of Ala Score and CIScore for the group ≦79 years old. r = 0.485,
P = 0.002.
結果
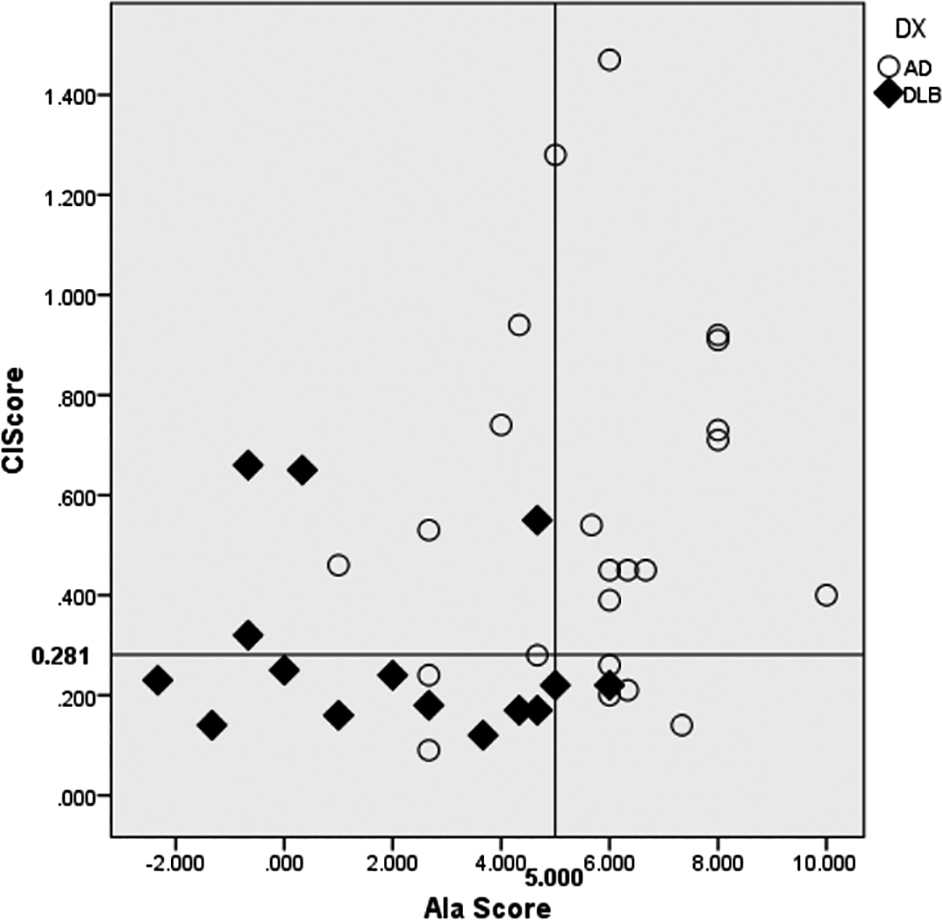
(1)79歳以下群39名でのAla ScoreとCIScoreの相関分析では,正の相関が見られた(r = 0.485, P = 0.002).Ala Scoreは5点未満8),CIScoreは0.281未満がDLBの可能性があるとされており6),今回の散布図ではその範囲内に70%(20名のDLB患者のうち14名)のDLBの患者が含まれていた(Fig. 1).一方で80歳以上の群38名ではAla ScoreとCIScoreの相関は見られなかった(r = 0.285, P = 0.083)(Fig. 2).
MMSE下位項目とCIScoreとの相関については,主要なものをTable 1に示す.79歳以下群と80歳以上群で,時間の見当識とCIScoreの間に負の相関が見られた.
Fig. 2
Scatter plot image of Ala Score and CIScore for the group of ≧80 years old. r = 0.285,
P = 0.083.
(2)年齢+疾患別群でのCIScoreとの相関は,79歳以下AD群ではAla ScoreとCIScoreの間に正の相関(r = 0.481, P = 0.037),79歳以下DLB群では時間の見当識とCIScoreの間に負の相関(ρ = –0.470, P = 0.036)が見られた.その他の主要な数値はTable 1に示す.
(3)既存のcut offとしてAla Scoreが5点未満,CIScoreが0.281未満をDLB陽性とした場合の全症例のAla Scoreの感度は0.800,特異度0.714,診断精度(正診率)0.753,AUC
0.822,CIScoreの感度は0.857,特異度0.690,診断精度0.766,AUC 0.842であった.群分けした感度,特異度については,Table 2に示す.
Table 2
Sensitivity, specificity, accuracy ratio, area under the curve for each group.
|
|
≦79 yrs.
Ala Score
|
≧80 yrs.
Ala Score
|
≦79 yrs.
CIScore
|
≧80 yrs.
CIScore
|
≦79 yrs.
Ala Score
and CIScore
|
≧80 yrs.
Ala Score
and CIScore
|
Existing cut off
(n = 39)
|
Existing cut off
(n = 38)
|
Existing cut off
(n = 39)
|
Existing cut off
(n = 38)
|
Existing cut off
(n = 39)
|
Existing cut off
(n = 38)
|
|
Sensitivity
|
0.750
|
0.867
|
0.950
|
0.733
|
0.700
|
0.600
|
|
Specificity
|
0.737
|
0.696
|
0.684
|
0.696
|
0.895
|
0.870
|
|
Positive predictive value
|
0.750
|
0.650
|
0.760
|
0.611
|
0.875
|
0.750
|
|
Negative predictive value
|
0.737
|
0.889
|
0.929
|
0.800
|
0.739
|
0.769
|
|
Positive likelihood ratio
|
2.850
|
2.848
|
3.008
|
2.410
|
6.650
|
4.600
|
|
Negative likelihood ratio
|
0.339
|
0.192
|
0.073
|
0.383
|
0.335
|
0.460
|
|
False positive rate
|
0.263
|
0.304
|
0.316
|
0.304
|
0.105
|
0.130
|
|
False negative rate
|
0.250
|
0.133
|
0.050
|
0.267
|
0.300
|
0.400
|
|
Diagnostic accuracy
|
0.744
|
0.763
|
0.821
|
0.711
|
0.795
|
0.763
|
|
AUC
|
0.792
|
0.868
|
0.925
|
0.757
|
0.934
|
0.901
|
|
|
≦79 yrs.
Ala Score
|
≧80 yrs.
Ala Score
|
≦79 yrs.
CIScore
|
≧80 yrs.
CIScore
|
≦79 yrs.
Ala Score
and CIScore
|
≧80 yrs.
Ala Score
and CIScore
|
Optimal cut off
(n = 39)
|
Optimal cut off
(n = 38)
|
Optimal cut off
(n = 39)
|
Optimal cut off
(n = 38)
|
Optimal cut off
(n = 39)
|
Optimal cut off
(n = 38)
|
|
Sensitivity
|
0.650
|
0.867
|
0.750
|
0.667
|
0.400
|
0.533
|
|
Specificity
|
0.789
|
0.696
|
0.947
|
0.783
|
0.947
|
0.913
|
|
Positive predictive value
|
0.765
|
0.650
|
0.938
|
0.667
|
0.889
|
0.800
|
|
Negative predictive value
|
0.682
|
0.889
|
0.783
|
0.783
|
0.600
|
0.750
|
|
Positive likelihood ratio
|
3.088
|
2.848
|
14.250
|
3.067
|
7.600
|
6.133
|
|
Negative likelihood ratio
|
0.443
|
0.192
|
0.264
|
0.426
|
0.633
|
0.511
|
|
False positive rate
|
0.211
|
0.304
|
0.053
|
0.217
|
0.053
|
0.087
|
|
False negative rate
|
0.350
|
0.133
|
0.250
|
0.333
|
0.600
|
0.467
|
|
Diagnostic accuracy
|
0.718
|
0.763
|
0.846
|
0.737
|
0.667
|
0.763
|
79歳以下のAla Scoreは感度0.750,特異度0.737.79歳以下のCIScoreは感度0.950,特異度0.684であった.検査の正確性を見る指標として,79歳以下群Ala
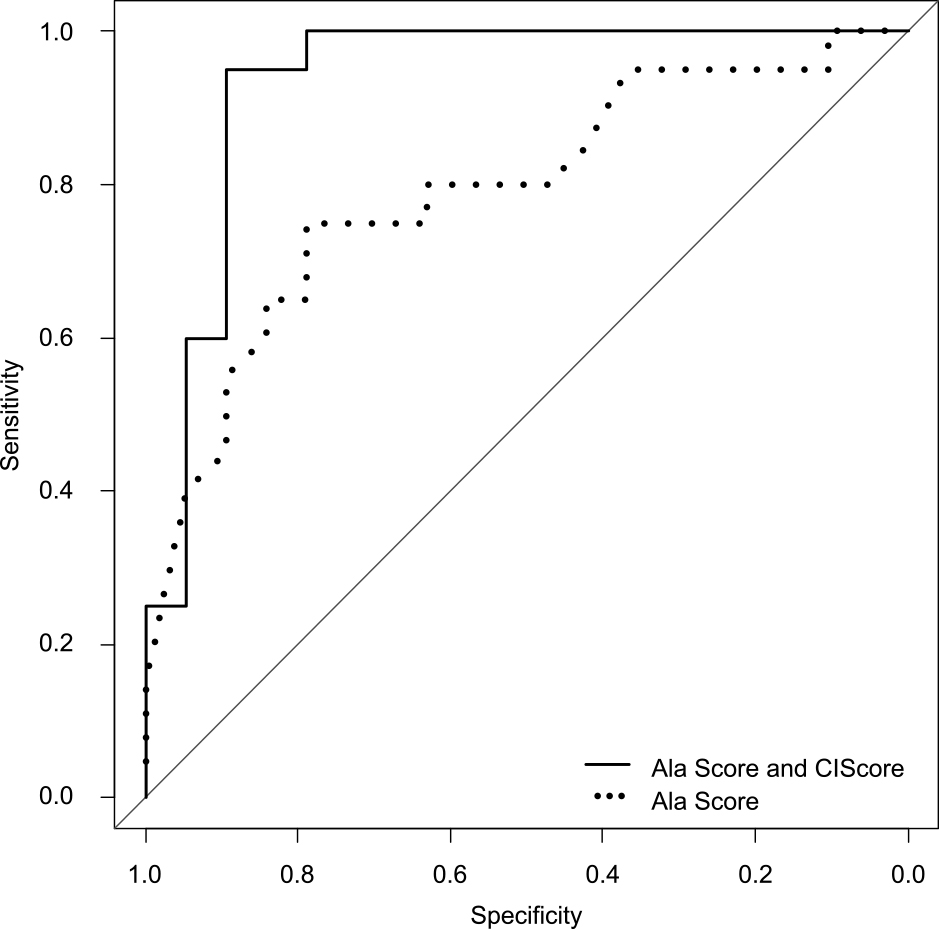
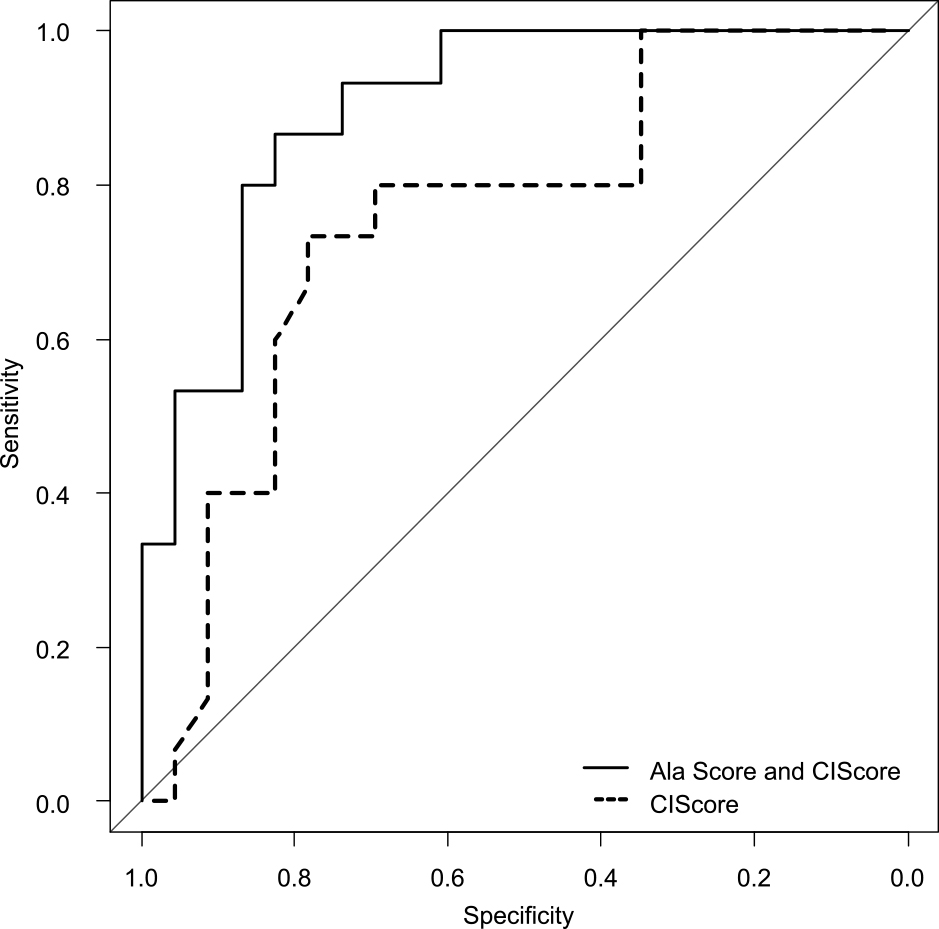
ScoreのAUCは0.792,79歳以下群CIScoreのAUCは0.925であった(Fig. 3).さらに,Ala Scoreが5点未満CIScoreが0.281未満(両方ともcut off値未満)の場合をDLB陽性とした場合の感度,特異度については,79歳以下群では,感度0.700,特異度0.895であった.79歳以下群で,Ala
ScoreとCIScoreを両方使って鑑別した場合のAUCは0.934であった.Ala ScoreのAUC 0.792とAla Score and CIScoreのAUC
0.934を比較した場合(Fig. 4),P値が0.0316となり,P < 0.05で二つのROC曲線のAUCは有意な差が認められた.
Fig. 3
ROC curve of Ala Score and CIScore for the group ≦79 years old. Ala Score Area Under
the curve (AUC): 0.792, CIScore AUC: 0.925.
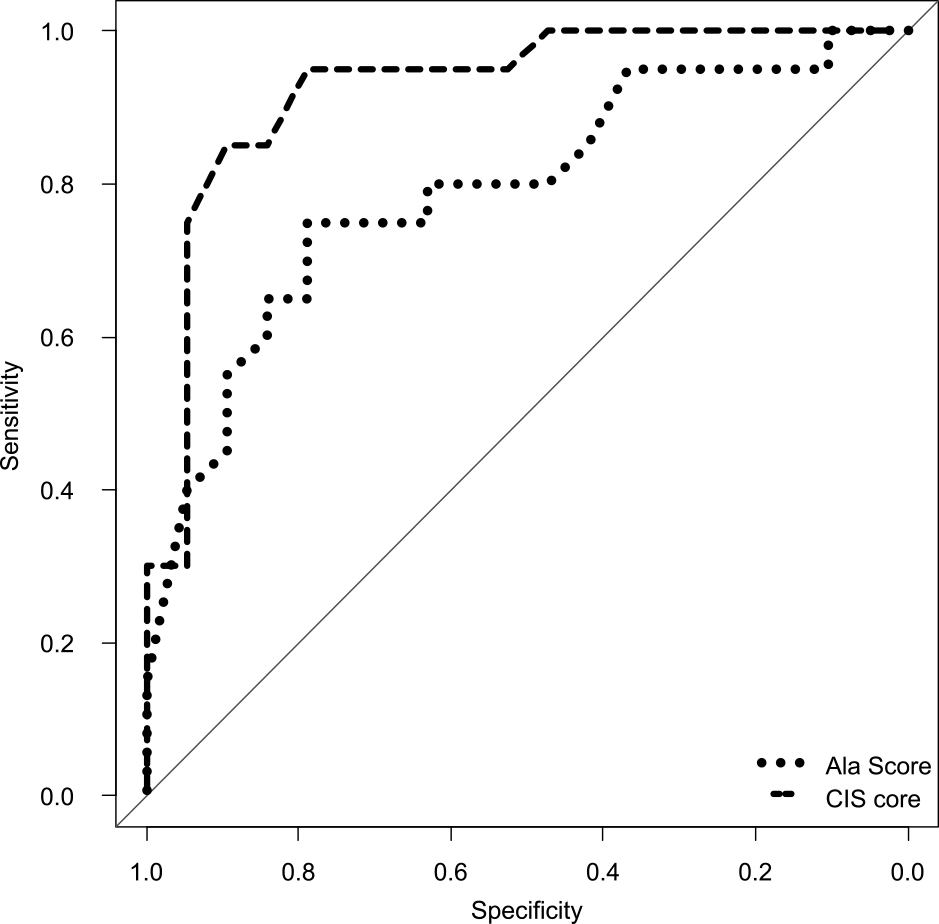
Fig. 4
ROC curve of Ala Score and “Ala Score and CIScore” for the group of ≦79 years old.
Ala Score AUC: 0.792, Ala Score and CIScore AUC: 0.934, P = 0.0316.
80歳以上のAla Scoreは感度0.867,特異度0.696.80歳以上のCIScoreは感度0.733,特異度0.696であった.80歳以上群Ala ScoreのAUCは0.868,80歳以上群CIScoreのAUCは0.757であった(Fig. 5).さらに,Ala Scoreが5点未満CIScoreが0.281未満(両方ともcut off値未満)の場合をDLB陽性とした場合の感度,特異度については,80歳以上群では,感度0.600,特異度0.870であった.80歳以上群で,Ala
ScoreとCIScoreを両方使って鑑別した場合のAUCは0.901であった.CIScoreのAUC 0.757とAla Score and CIScoreのAUC
0.901を比較した場合(Fig. 6),P値が0.0473となり,P<0.05で二つのROC曲線のAUCは有意な差が認められた.
Fig. 5
ROC curve of Ala Score and CIScore for the group ≧80 years old. Ala Score AUC: 0.868,
CIScore AUC: 0.757.
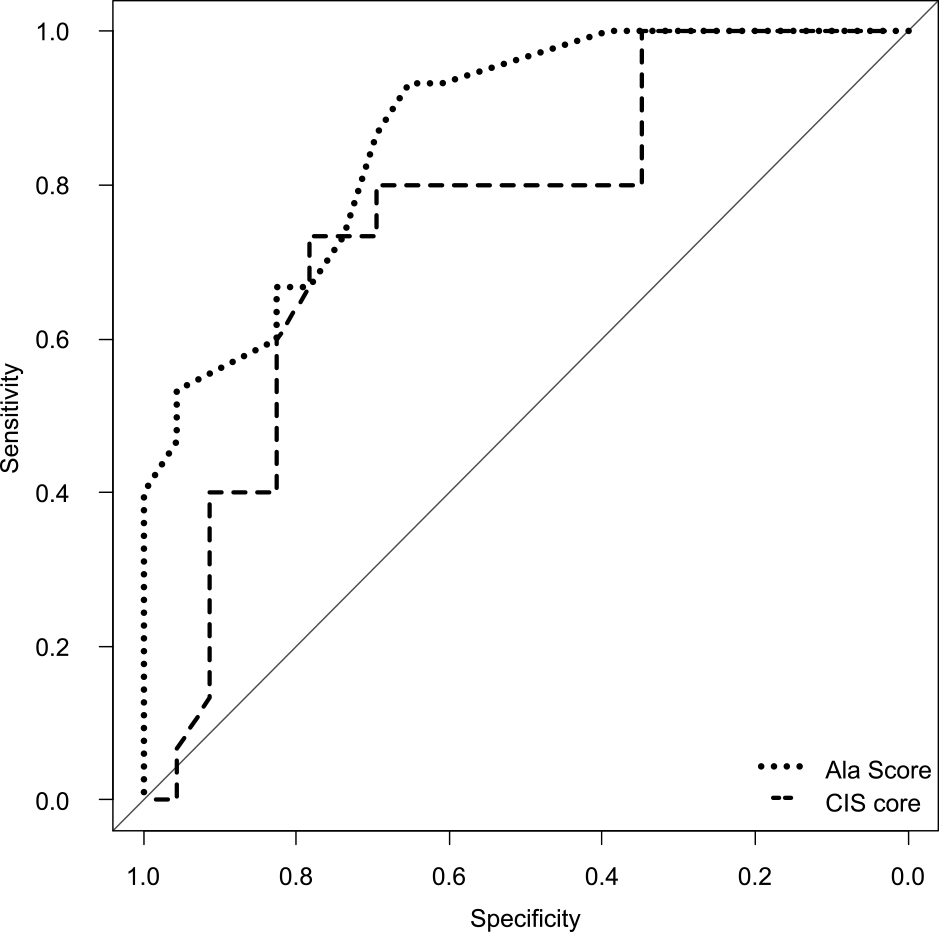
Fig. 6
ROC curve of CIScore and “Ala Score and CIScore” for the group ≧80 years old. CIScore
AUC: 0.757, Ala Score and CIScore AUC: 0.901, P = 0.0473.
また,CIScoreについては設定すべきcut off値について,各施設での確認が必要との報告もある7)ため,EZRによって算出された最適cut off値(感度+特異度が最大になるcut値)についても感度,特異度,診断精度の検討を行った(Table 2).79歳以下の最適cut off値は,Ala Score 4.333,CIScore 0.240,80歳以上の最適cut off値は,Ala Scoreは5.000と既存のcut
off値と変わらず,CIScoreは0.250であった.比較すると,感度は既存のcut offの方が良く,診断精度は79歳以下,80歳以上のCIScoreについては最適cut off値の方がやや高かった.
考察
Ala Score8)とCIScore6)の両者ともにDLBの鑑別を目的とするマーカーであるが,我々の研究ではこれら二つの数値には79歳以下の群で相関があることが判明した.したがって,79歳以下群はSPECTが施行できない施設でAla
Scoreが代替検査となり得る可能性が示唆された.また,今回の79歳以下の群の散布図では,DLB鑑別の既存のcut off値である「Ala Score 5点未満,CIScore
0.281未満」の範囲内に70%のDLBの患者が含まれた.一方で80歳以上の群ではAla ScoreとCIScoreの相関は見られず,80歳以上DLB群では,CIScoreの平均が0.29とcut
off値を上回っており,散布図や感度の結果からも,79歳以下の群と比較して,80歳以上の群はCIScoreによる鑑別が難しくなることが示唆された.この一つの要因としては,高齢のDLBには,よりAD病理の合併が併存することが多く,それが画像マーカーに反映される可能性が高くなるためと推測される.
ADとDLBの合併
DLB病理の検討で小阪の提唱するpure formは極めて稀で,通常はcommon formすなわち軽いAD病理変化が合併している症例が多い11).またAD患者の脳血流SPECTを若年,老年,超高齢の3群に分けて健常コントロール群と比較検討した研究では,高齢となるほど後部帯状回~楔前部,側頭頭頂葉の血流低下が軽度で一方,前頭葉,側頭葉内側の血流低下がより明らかになり,ADの典型的血流パターンとは異なってくると指摘している12).
DLB患者の2年間の追跡ではCIS比(後部帯状回/楔前部+楔部)は,軽度のDLBが進行しMMSEが低下するにつれてCISが減少し,CIS比とMMSEスコアの関係は逆U字型であった13).Prodoromal DLBの状態では,後部帯状回の血流は保たれて,分母の後頭葉の血流低下はめだたないためCIS比の増加は乏しい.その後分母の後頭葉の血流低下が顕著になるとCIS比は増加し,やがてMMSEの低下に伴い分子の後部帯状回の血流低下も見られるようになると再びADパターンの数値になることが考えられる7).
ADの発生率は80歳以降に著しく増加したとの報告もあり14),今回の研究で様々な年齢での群分けを試みたが,80歳をカットオフ値とすることが79歳以下CIScoreの感度,80歳以上のAla Scoreの感度も高く,DLBとADの鑑別の点でよいと思われた.
時間の見当識と関連する脳領域
今回,時間の見当識について79歳以下(AD + DLB)群,80歳以上(AD + DLB)群,79歳以下DLB群で,MMSEの時間の見当識とCIScoreとの間に負の相関が見られた.時間の見当識の平均点は79歳以下DLB群が4.25と最も軽症で,そこから80歳以上DLB群3.67,79歳以下AD群3.26,80歳以上AD群2.57という順に悪化が見られる.つまり,DLBは見当識が保たれ,ADは初期から見当識が低下し年齢とともに悪化する.帯状回と楔前部は時間の見当識と関連があり15)~17),ADはこの脳領域の代謝,血流の低下に伴い,時間の見当識が低下し,DLBはこの脳領域が比較的保たれ,時間の見当識が保たれていることと関連する.また年齢に加え疾患別で群分けした際に,79歳以下DLB群で時間の見当識とCIScoreで負の相関が見られ,その他の年齢疾患群で相関がなかったことは,若年のDLB患者は時間の見当識が保たれ,その程度は帯状回と楔前部の血流と関連することを示唆している.
遅延再生と計算
今回の症例解析でのMMSE下位項目点数の平均値の結果は,ADと比べてDLBは遅延再生が比較的保たれており,計算と図形が低いという典型的な結果を示していた.遅延再生平均は79歳以下群ではAD
0.89,DLB 1.20,80歳以上群ではAD 0.70とDLB 1.27でDLBは年齢によって大きな差はないが,ADの遅延再生平均は80歳以上群の方がより低下していた.一方で計算平均は79歳以下群のAD
2.89,DLB 2.35に比較して,80歳以上群ではAD 2.52,DLB 1.40と両群共に低下していたがDLBでより著明に見られた.すなわちADは年齢によって大きな差はないが,DLBの計算平均は高齢になるとより低下するという結果となった.これらの要因により,Ala
Scoreの感度が80歳以上群でより高くなったと思われる.
Ala ScoreとCIScoreの感度,特異度,AUC
Ala ScoreとCIScoreは既存のcut offの場合,79歳以下群で相関が見られ,Table 2の結果から,79歳以下の場合は,Ala ScoreよりもCIScoreの方が,感度とAUCが高く,スクリーニングに適している一方,80歳以上の場合はCIScoreよりもAla
Scoreの方が,感度とAUCが高く,スクリーニングに適している.
さらに,Ala ScoreとCIScoreが両方とも既存のcut off値未満の場合をDLB陽性とすると,79歳以下群も,80歳以上群もAla ScoreあるいはCIScore単独で鑑別するよりも,特異度とAUCが高まり鑑別診断能が上がることが分かった.
また,79歳以下の患者も80歳以上の患者も,Ala Scoreが5点以上でCIScoreが0.281以上の場合はADである確率が高いことが分かった(Fig. 1, 2).
Ala ScoreやCIScoreは日常診療で可能な検査であり,心理検査と脳画像データの両者の検討により疾患鑑別の感度,特異度が向上する可能性が示唆された.
Notes
※著者全員に本論文に関連し,開示すべきCOI状態にある企業,組織,団体はいずれも有りません.
文献
McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies Fourth consensus report of the DLB Consortium. Neurology
2017;89:88-100.
Donnemiller E, Heilman J, Wenning GK, et al. Brain perfusion scintigraphy with 99mTc-HMPAO
or 99mTc-ECD and 123I-β-CIT single-photon emission tomography in dementia of the Alzheimer-type
and diffuse Lewy body disease. Eur J Nucl Med 1997;24:320-325.
Pasquier J, Michel BF, Brenot-Rossi I, et al. Value of 99mTc-ECD SPET for the diagnosis
of dementia with lewy bodies. Eur J Nucl Med 2002;29:1342-1348.
Perneczky R, Drzezga A, Boecker H, et al. Cerebral metabolic dysfufunction in patients
with dementia with Lewy bodies and visual hallucinations. Dement Geriatr Cogn Disord
2008;25:531-538.
Nagahama Y, Okina T, Suzuki N, et al. Neural correlates of psychotic symptoms in dementia with Lewy bodies. Brain 2010;133:557-567.
Imabayashi E, Soma T, Sone D, et al. Validation of the cingulate island sign with
optimized ratios for discriminating dementia with Lewy bodies from Alzheimer’s disease
using brain perfusion SPECT. Ann Nucl Med 2017;31:536-543.
今林悦子. Cingulate island sign. Brain Nerve 2018;70:879-888.
Ala TA, Hughes LF, Kyrouac GA, et al. The Mini-Mental State exam may help in the differentiation
of dementia with Lewy bodies and Alzheimer’s disease. Int J Geriatr Psychiatry 2002;17:503-509.
McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s
disease: recommendations from the National Institute on Aging-Alzheimer’s Association
workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 2011;7:263-269
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical
statistics. Bone Marrow Transplantation 2013;48:452-458.
髙尾昌樹.神経病理学的観点からみたレヴィ小体型認知症とアルツハイマー病との合併.Brain Nerve 2018;70:905-913.
平尾健太郎,羽生春夫,金高秀和ら.脳血流SPECTによる超高齢アルツハイマー病の脳血流パターンの特徴.日老医誌 2008;45:408-413.
Iizuka T, Iizuka R, Kameyama M. Cingulate island sign temporally changes in dementia
with Lewy bodies. Sci Rep 2017;7:14745.
Dodge HH, Bracchio TJ, Fisher GG, et al. Trends in the prevalence of dementia in
Japan. Int J Alzheimers Dis 2012;2012:956354.
Hirono N, Mori E, Ishii K, et al. Hypofunction in the posterior cingulate gyrus correlates
with disorientation for time and place in Alzheimer’s disease. J Neurol Neurosurg
Psychiatry 1998;64:552-554.
Peer M, Salmon R, Goldberg I, et al. Brain system for mental orientation in space,
time, and person. Proc Natl Acad Sci U S A 2015;112:11072-11077.
Vann SD, Aggleton JP, Maguire EA. What does the retrosplenial cortex do? Nat Rev
Neurosci 2009;10:792-802.