CQ 1
What kinds of patients receive treatment by self-injection of sumatriptan at home (indication, adverse effects, contraindications)?
Recommendation
Self-injection of sumatriptan at home is indicated for patients with a definitive diagnosis of migraine or cluster headache. Cluster headache may be considered the best indication for self-injection of sumatriptan at home, because of its fast-acting feature and convenience. Migraine is an indication when severe attacks cause severe disability in daily and social lives, or when frequent vomiting impedes administration of oral medications. The safety of this treatment has not been established in children. This treatment has to be used with caution in elderly persons.
The major adverse effects include nausea, chest discomfort, palpitation, bleeding at injection site, malaise, and somnolence.
This treatment should not be given to patients with familial hemiplegic migraine, sporadic hemiplegic migraine, basilar-type migraine (migraine with brainstem aura), or ophthalmoplegic migraine; patients with a history of heart disease, cerebrovascular disorders, or periphery circulatory disturbance; patients with uncontrolled hypertension; patients with server liver disorder; and patients on treatment with monoamine oxidase (MAO) inhibitor or within 2 weeks after discontinuation. For patients who are prescribed sumatriptan self-injection while also taking oral ergotamine or triptans other than sumatriptan, they should be instructed to use the two agents separately with an interval of at least 24 hours.
| Grade A |
Background and Objective
Subcutaneous injection of sumatriptan is an effective treatment for cluster headache attacks. However, attacks occur frequently at night, when seeking treatment at a medical facility is difficult. Moreover, the headache duration is relatively short. Even if a patient visits a medical facility during attack, often the headache has improved by the time the patient is seen by a doctor. Also, visiting a medical facility is difficult in the case of severe migraine attack, especially when accompanied by vomiting. During severe headache attack, self-injection of sumatriptan at home is a fast acting and convenient treatment modality. This section examines what kind of patients can use sumatriptan self-injection at home safely.
Comments and Evidence
Since cluster headache attacks are accompanied by severe pain of relatively short duration (50 to 180 min) compared to migraine, self-injection of sumatriptan at home that can stop the pain as soon as attack occurs is an effective treatment. To make a definitive diagnosis of cluster headache, it is important to differentiate from secondary headache caused by paranasal sinus, pituitary and other disorders.
For migraine, the best indication for self-injection of sumatriptan at home is patients who have very severe attacks, such as those who have a history of being transported to emergency department, and who respond to sumatriptan injection. The treatment is especially indicated for patients who have associated symptom of repeated vomiting, making oral administration difficult. However, before deciding whether to prescribe self-injection of sumatriptan at home, ensure that adequate treatments including conventional oral medications and other concomitant medications have been implemented, and confirm in a medical institution that the patient responds to sumatriptan injection.
According to the experience of clinical use of 7000 cases in Japan, sumatriptan injection is as highly effective as the tablet and nasal spray formulations, and is safe.1) In a postmarketing surveillance of sumatriptan self-injection (Imigran Kit Subcutaneous Injection 3 mg) conducted in Japan, the treatment was effective in 92 of 103 patients (89.3%) with migraine and in 60 of 60 patients (100%) with cluster headache, showing high response rates. Adverse reactions were observed in 28 of 173 patients (16.2%), and the major adverse reactions were nausea (3.5%), chest discomfort (2.9%), palpitation (2.3%), bleeding at injection site (1.7%), malaise (1.7%) and somnolence (1.7%). None of the events were serious. These result confirmed high effectiveness and safety of this product.2)
No case-control study on sumatriptan subcutaneous injection in children has been reported. In an open-study of sumatriptan subcutaneous injection in children and adolescents with migraine, response was observed in 64 to 78% of the patients, but adverse reactions occurred in approximately 80% of the patients.3) In children, due to the predicted difficulties in identifying symptoms and handling the subcutaneous injection kit, self-injection is not recommended.
Regarding the risk of heart disease after sumatriptan administration, sumatriptan is a vasoactive drug and theoretically is predicted to cause vasoconstriction. In a study on chest oppression and electrocardiographic changes after sumatriptan injection, no ST changes were observed.4) A report indicates that use of triptans in patients with no coronary disease does not increase the risk of serious cardiovascular events.5) A literature review of 32 cases in which vascular events occurred after triptan administration identified few cases with a definite causal relationship with triptan.6) The above findings thus suggest a very low risk of cardiovascular or cerebrovascular events caused by triptan. However, triptans should be used with caution in patients with risk factors.
• Precautions in prescription
(1) First of all, exclude secondary headaches, and perform a definitive diagnosis for cluster headache or migraine.
(2) Only prescribe to patients who can judge that they have migraine or cluster headache.
(3) Prescribe to patients who have a good understanding of self-injection at home.
(4) In principle, there is no need to switch to this treatment if headache is controlled by the medications already prescribed.
(5) For migraine patients who do not respond adequately to oral or nasal spray formulations, there is a possibility that they are missing the timing of using the medication early after onset. Before switching to sumatriptan self-injection, the patients should be given thorough guidance on early use of medications.
When prescribing, bearing in mind that due to the characteristic of the formulation, blood level increases rapidly during administration and adverse reactions not seen with oral or nasal spray formulations may appear.
(7) In principle, do not prescribe to patients who feels resistance or anxiety toward “injections”.
(8) In many Western countries, this treatment is not recommended for children (aged 18 or younger) and elderly patients (aged 65 or above). In Japan, the package insert states that “safety is not established” for children, and “use with caution” for elderly patients. Greater caution is needed.
• References
1) Takeshima T, Igarashi H, Hamada J, Shimizu T, Ishida A, Yokomori J, Nagata D: Postmarketing surveillance of sumatriptan formulations (Imigran Injection, tablet, nasal spray) for migraine or cluster headache: from the data collected from 7,000 cases. Diagnosis and Treatment 2006; 94(11): 2149-2168. (In Japanese)
2) Shimizu T, Sakai F, Tanaka R, Kato M, Ijiri S: Postmarketing surveillance of sumatriptan self-injection for migraine and cluster headache. J New Rem & Clin 2010; 59(5): 770-784. (In Japanese)
3) Lewis D, Ashwal S, Hershey A, Hirtz D, Yonker M, Silberstein S; American Academy of Neurology Quality Standards Subcommittee; Practice Committee of the Child Neurology Society: Practice parameter: pharmacological treatment of migraine headache in children and adolescents: report of the American Academy of Neurology Quality Standards Subcommittee and the Practice Committee of the Child Neurology Society. Neurology 2004; 63(12): 2215-2224.
4) Tomita M, Suzuki N, Igarashi H, Endo M, Sakai F: Evidence against strong correlation between chest symptoms and ischemic coronary changes. after subcutaneous sumatriptan injection. Intern Med 2002; 41(8): 622-625.
5) Dodick D, Lipton RB, Martin V, Papademetriou V, Rosamond W, Maassen VanDenBrink A, Loutfi H, Welch KM, Goadsby PJ, Hahn S, Hutchinson S, Matchar D, Silberstein S, Smith TR, Purdy RA, Saiers J; Triptan Cardiovascular Safety Expert Panel: Consensus Statement: Cardiovascular safety profile of triptans(5-HT1B/1D agonists) in the acute treatment of migraine. Headache 2004; 44(5): 414-425.
6) Chalaupka FD: Acute myocardial infarction with sumatriptan: a case report and review of the literature. Headache 2009; 49(5): 762-764.
• Search terms and secondary sources
• Search database: PubMed
sumatriptan & injection 407, sumatriptan & injection & self 34
• Search database: Ichushi Web for articles published in Japan
sumatriptan & subcutaneous injection 94
sumatriptan & self injection 24
CQ 2
How should self-injection of sumatriptan at home be initiated and explained to the patient? What is the appropriate amount to be prescribed?
Recommendation
Initiation of self-injection of sumatriptan at home starts when the doctor prescribes the drug to the patient who is judged to be capable of using self-injection properly. At the time of prescription, provide patient education including method of use. Use “Imigran Kit Subcutaneous Injection 3 mg Training Set” to instruct and explain to patients. Explain in detail the adverse effects that may occur by self-injection of this drug. Instruct patients to follow doctor’s directions if any abnormality occurs after self-injection. Also instruct the patients on appropriate method to dispose of the used injection product.
Since sumatriptan is highly effective and fast acting, self-injection of sumatriptan is recommended for patients with migraine or cluster headache who do not respond adequately to other treatments. Prescribe an appropriate amount taking into consideration for use on an as-needed basis.
For migraine, the amount of each prescription is two kits (4 ampoules) to five kits (10 ampoules). However, for patients who have difficulties with frequent hospital visits, it is possible to prescribe an amount deemed appropriate considering the severity and frequency of attacks. For cluster headache, the amount of each prescription is usually 7 kits (14 ampoules).
| Grade A |
Background and Objective
In order that self-injection of sumatriptan at home is used safely and properly, it is important to provide detailed and accurate guidance and explanations at the time of initiation.
Some patients with migraine or cluster headache do not obtain satisfactory result with oral medications alone. These patients can be prescribed self-injection drugs for the purpose of treatment. When using this treatment, it is important to accurately predict the effectiveness and safety in order to accomplish the goal. Prescription should be decided upon considering concomitant use with existing treatments and the general health insurance rules.
Comments and Evidence
Initiation of self-injection and explanation to patients
There are few reports on the initiation of self-injection of sumatriptan at home and explanations to patients. In a study comparing the practicality of a pen-type injector included in the sumatriptan injection kit and the conventional autoinjector for sumatriptan, 80% of the responders rated the pen-type injector as “very easy” or “easy” to use.1) Furthermore, 75% of the patients already using autoinjector reported that explanation of the pen injector took less than 5 minutes. The report concluded that subcutaneous injection can be done even during severe migraine attacks. Although the above report indicates that self-injection of sumatriptan at home is easy to use, it is necessary to conduct adequate patient education before initiating treatment.
1. Method of explanation to patient using the training set
A doctor or a nurse who has good understanding of the safety and effectiveness of self-injection of sumatriptan at home, and is capable of giving sufficient guidance on the use of this treatment to the patients should provide appropriate guidance and explanations.
Use the “Imigran® Kit Subcutaneous Injection 3 mg Training Set”2) when giving guidance or explanation to patients.2) Following the “Start Manual”, and explain based on “Instructions for Practice”. If necessary, use the “Use Instruction DVD” and “Points for Explaining to Patients”.
Make sure to check how much the patient has learned using the “Training Checklist for Use in Medical Institution”. When team care is practiced, decide the roles of team members; such as, the nurse explains the process of self-injection of this drug and the doctor checks whether the patient can use the drug properly. This will also allow double checking and reduce the burden on doctors.
In addition, various approaches have to be used to increase patient’s understanding, such as asking the patient to practice by him/herself using kits for practice.
2. Method of initiation training
Initiation training for patient should be conducted repeatedly during each visit or admission, until the patient is judged to have acquired the competence of self-injecting sumatriptan at home. The number of training sessions required varies depending on the patient’s degree of understanding. Since it may take some time from prescription to actually using the drug, give a starter pack to the patient at the time of prescription, and instruct him/her to practice at home.
3. Method of disposal of used cartridge packs
At the time of prescription, instruct the patient on the method of disposal of used cartridge packs. The disposal method differs depending on the rules of the municipality in which the patient lives. Instruct the patient to make inquiries at the municipality. Inquiry should be made to the department that handles waste disposal and recycling, at the municipality nearest to the patient’s residence.
There are mainly three methods of waste disposal:
(1) If disposal as general waste (combustible waste or non-combustible waste for landfill) is possible, the patient can dispose at their own home
(2) If disposal as general waste (as above) is not possible, bring back to the medical institution that prescribed the drug.
(3) If disposal method is not known or cannot be confirmed even after inquiring to the municipality, bring back to the medical institution that prescribed the drug.
The amount to be prescribed
For migraine, common attacks are often controlled by oral or nasal spray triptans, and sumatriptan self-injection is usually used when oral medication is difficult due to severe vomiting, when attack starts during sleep at night and the patient is awaken by the pain, or when oral or nasal spray administration is delayed and attack becomes severe. As long as the patient is receiving appropriate treatment, an increase in number of self-injection is not expected. A study investigating the migraine attack frequency reported that 52% had an attack frequency of around once a month.3) The proportions of patients with headache frequency of 1 to 7 days a year were reported to be 52.6% for migraine with aura,4) and 37.9%4) or 40%5) for migraine without aura. Therefore, considering also consecutive days off, one prescription of 2 kits (4 ampules) may be appropriate. However, since patients may have difficulties visiting hospitals, one prescription from 2 kits (4 ampules) up to 5 kits (10 ampules) is recommended. In patients with frequent severe attacks, prescription of an amount deemed appropriate to the patient is possible.
For cluster headache, the attack frequency is once every other day to eight times a day according to the ICHD-II diagnostic criteria. A study investigating the attack frequency reported that the most common frequency was 4 or 5 times a day.6) Another study reported a mean attack frequency of 1.67 times a day, while most patients had attacks once to 4 times a day.7) Based on the above findings, assuming an attack frequency of 2 times per day and conforming to the number of prescription days for other as-needed medications, a prescription for 7 days seems suitable. Hence, prescribing a maximum of 7 kits (14 ampules) is considered appropriate. Moreover, the cluster period for cluster headache has been reported to be 8.6 weeks on average,6) and usually continues for 1 to 2 months. Therefore, a maximum of four prescriptions a month is required.
The explanatory leaflet and confirmation leaflet are shown in Figures 1 and 2, respectively.
General principle for guidance and management fees for home care
(1) “Guidance and management fees for home care” is computed in the case of the following: for a patient in whom a doctor has judged that the above-mentioned guidance and management are necessary and appropriate, the above-mentioned doctor gives guidance and appropriate advice to the patient or the person who cares for the patient; provides adequate medical management of the patient; conducts guidance regarding the methods of home care, matters requiring attention, and measures during emergency; and supplies necessary and adequate amounts of hygienic materials or insurance-covered medical materials.
(2) The above-mentioned medical institution (authorized to treat patients under health insurance coverage) should supply the patients with materials for disinfection (such as alcohol cotton swab) needed to conduct self-injection, in an amount deemed necessary and appropriate, and calculated as part of the guidance and management fees for home care
• References
1) Gbel H, Baar H, Beikfner HD, Bhme K, Beckmann-Reinhold A: Practicability and acceptance of subcutaneous self-administration of the selective serotonin agonist sumatriptan. Headache 1998; 38(4): 267-269.
2) Package insert for Imigran® Kit Subcutaneous Injection 3 mg. (In Japanese)
3) Nikiforow R: Headache in a random sample of 200 persons: a clinical study of a population in northern Finland. Cephalalgia 1981; 1(2): 99-107.
4) Rasmussen BK, Olesen J: Migraine with aura and migraine without aura: an epidemiological study. Cephalalgia 1992; 12(4): 221-228.
5) Rasmussen BK, Jensen R, Schroll M, Olesen J: Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol 1991; 44(11): 1147-1157.
6) Bahra A, May A, Goadsby PJ: Cluster headache: a prospective clinical study with diagnostic implications. Neurology 2002; 58(3): 354-361.
7) Russell D: Cluster headache: severity and temporal profiles of attacks and patient activity prior to and during attacks. Cephalalgia 1981; 1(4): 209-216.
• Search terms and secondary sources
• Search database: PubMed (2011/12/22)
“sumatriptan” “self administration” Limits Activated: Clinical Trial 29
“migraine” “attack” “frequency” 431
“cluster headache” “attack” “frequency” 75
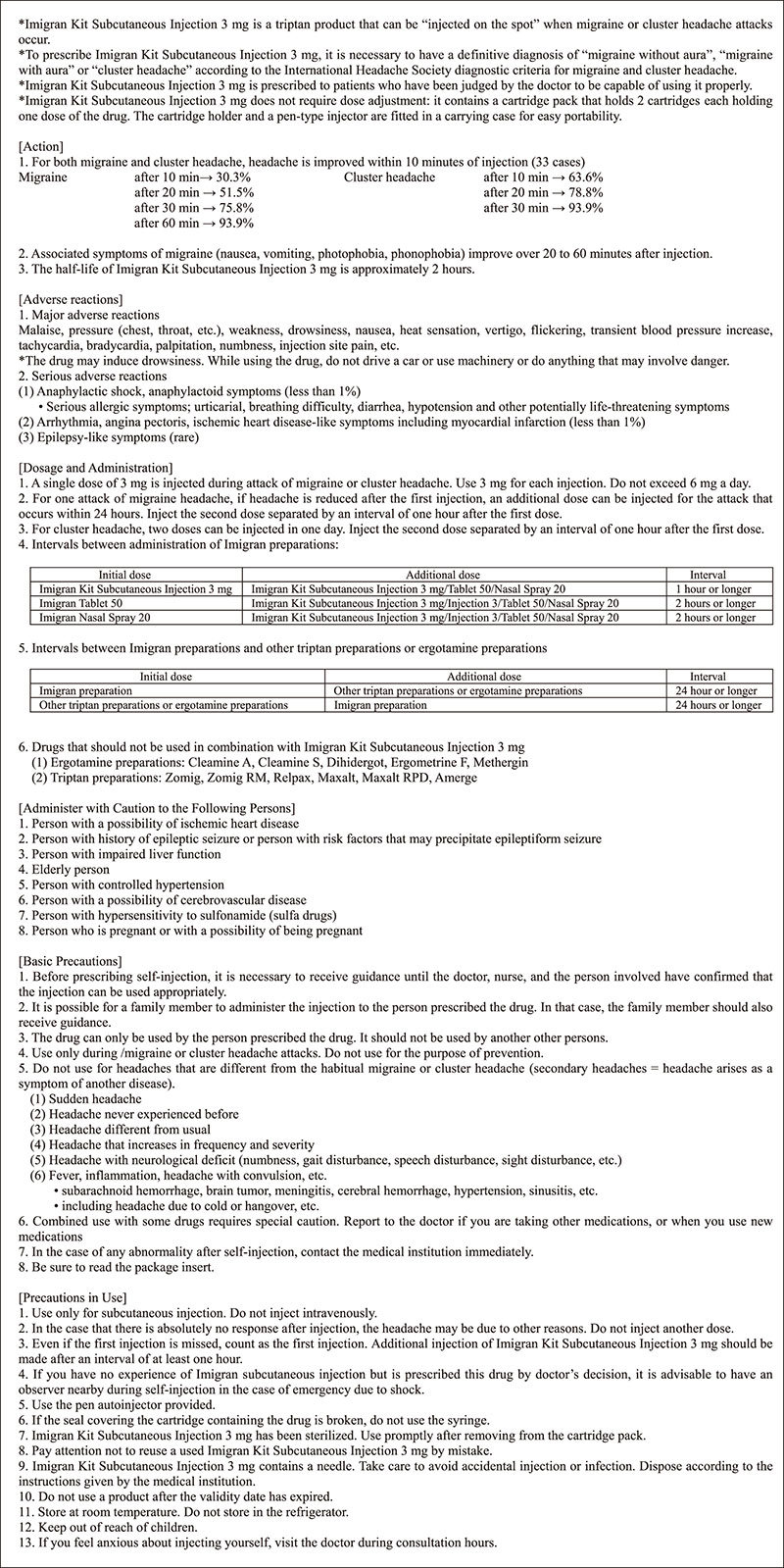
Figure 1. Self-injection of Imigran® Kit Subcutaneous Injection 3 mg
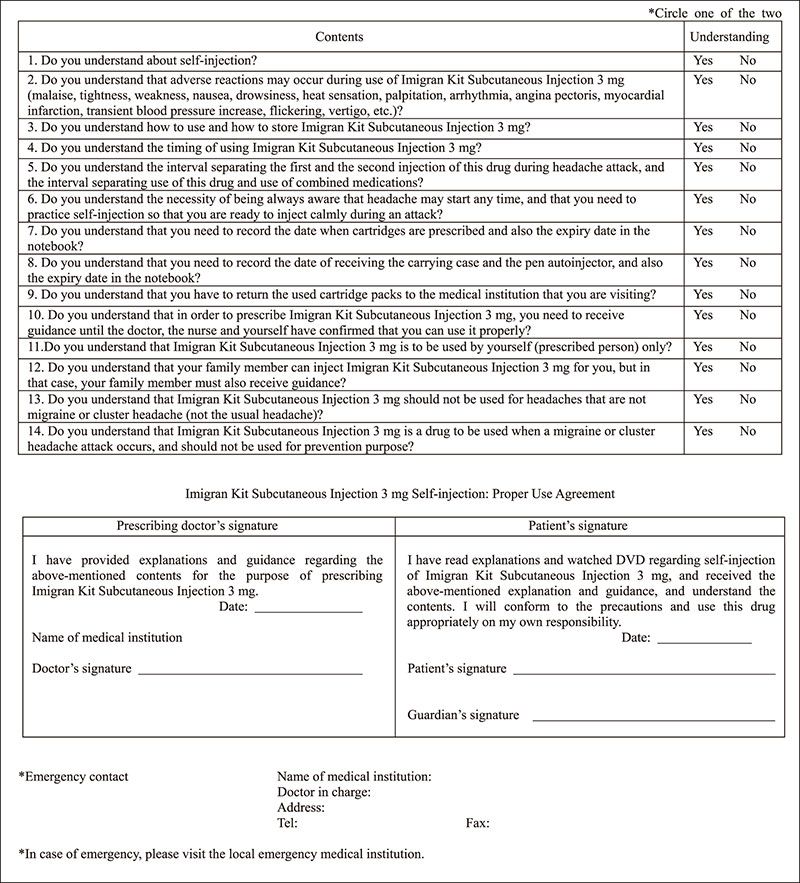
Figure 2. Items to confirm proper use of Imigran® Kit Subcutaneous Injection 3 mg self-injection.
CQ 3
What instructions should be given for the first sumatriptan self-injection at home, and what measures should be taken during emergency (when serious adverse event occurs)?
Recommendation
For patient who has never received sumatriptan subcutaneous injection and patient who self-injects at home for the first time, instruct the patient to inject in the presence of an observer such that contact with a medical institution is possible in case of emergency. For self-injection of sumatriptan at home, instruct the patient about the adverse events that may occur and the method of access to medical institutions, in order to be prepared for the occurrence of serious adverse events.
| Grade A |
Background and Objective
Serious adverse events of sumatriptan subcutaneous injection are very rare, but anaphylactic shock and myocardial infarction have been reported.1) When a patient self-injects sumatriptan at home for the first time, anxiety over the technique and adverse events is anticipated. Therefore, this section verifies the desirable approach for first time use. Other emergencies may occur, such as when sumatriptan is used by mistake for secondary headaches or other conditions. This section also examines the measures to be taken in emergency situations (when serious adverse events occur) and precautions to take foreseeing the occurrence of emergencies, and presents the recommended methods.
Comments and Evidence
Some articles from overseas have reported serious adverse events associated with sumatriptan 6 mg subcutaneous injection, such as myocardial infarction, cerebrovascular disorder, and allergic reactions, but at a very low incidence of less than 1% for anaphylactic shock or anaphylactoid symptoms, and less than 1% for arrhythmia, angina pectoris or ischemic heart disease-like symptoms such as myocardial infarction.1)-3) For sumatriptan 3 mg subcutaneous injection that became available in Japan since 2000, serious adverse events are extremely rare.4) In a clinical trial of sumatriptan self-injection conducted in Japan, the incidence of adverse reactions was 11 of 66 subjects (16.7%), and the major adverse reactions included malaise 4.5%, asthenia 3.0%, and chest discomfort 3.0%.5) According to the post-marketing surveillance conducted in Japan, adverse reactions were found in 28 of 173 patients (16.2%), and the major reactions included nausea, chest discomfort, and palpitation, none of which were serious. Among 173 patients, only 2 of 110 migraine patients and 2 of 63 cluster headache patients had used sumatriptan before being prescribed the kit product, while the vast majority of the patients had no experience of use. These results suggest that even in patients with no experience of using sumatriptan injection, there is a low risk of serious adverse reactions.6)7) Evaluation of proper usage showed high rates of proper usage in both migraine patients (99.1%) and in cluster headache patients (98.4%).6) In a study on the practicality of a kit product by Gobel et al.8), 80% of the patients evaluated the kit to be easy to use or very easy to use. With adequate prior explanations and practice, there seems to be little technical problem.
When a patient self-injects sumatriptan for the first time, anxiety over the technique and adverse events is anticipated. In Japan, a randomized controlled trial (RCT) of self-injection kit used at home was conducted recruiting migraine patients who had received sumatriptan injection for migraine attacks within one year, and cluster headache patients irrespective of treatment history. After receiving adequate guidance on self-injection and undergoing mock injection, these patients self-injected at home for the RCT.5)
In overseas clinical trials of self-injection kits, patients with no experience of using sumatriptan self-injected at home after giving detailed instructions.9)10) Since serious adverse events such as anaphylactic shock and myocardial infarction occur not only during the first injection, constant attention is necessary. For the first injection at home, detailed instructions should be given beforehand, and it is advisable to perform the injection in the presence of an observer in case of emergency. For patients with strong anxiety toward the technique or adverse events and patients with a history of allergy, a recommended option to initiate self-injection is to admit the patients into hospitals or let patients self-inject under supervision of medical personnel in outpatient or emergency department.
Headache attacks that differ in severity from the usual migraine or cluster headache may be secondary headaches such as subarachnoid hemorrhage, intracerebral hemorrhage, and cerebral infarction, and appropriate measures have to be taken. Before prescription, patients should be given instructions and information to seek emergency care at a medical institution when serious adverse events occur or when secondary headache that differs from the usual headache is suspected.
Medical institutions that have 24-hour emergency service should give information and instructions to patients self-injecting at home to seek emergency care when emergency situation occurs, and should clearly state in the medical records that the patients are self-injecting sumatriptan at home. Medical institutions that cannot provide immediate care during night time or emergency (such as clinics and medical institutions located far from the patients’ residence) should collaborate with medical institutions that can accept emergency cases, and should explain this to the patients. Since emergency may occur during travelling or in work locations, patients should be instructed to bring along a sumatriptan kit together with a referral letter to the attending doctor or a card recording relevant information as an aid to provide information when the patients visit the nearest medical institution in case of emergency.
• References
1) Package insert of Imigran Kit Subcutaneous Injection 3 mg. Revised in October 2010 (3rd edition). (In Japanese)
2) Gawel MJ, Worthington I, Maggisano A: A systematic review of the use of triptans in acute migraine. Can J Neurol Sci 2001; 28(1): 30-41.
3) Dahlf CG, Saiers J: Sumatriptan injection and tablets in clinical practice: results of a survey of 707 migraineurs. Headache 1998; 38(10): 756-763.
4) Takeshima T, Igarashi H, Hamada J, Shimizu T, Ishida A, Yokomori J, Nagata D: Postmarketing surveillance of sumatriptan formulations (Imigran Injection, Tablet, Nasal Spray) for migraine or cluster headache: from the data collected from 7,000 cases. Diagnosis and Treatment 2006; 94(11): 2149-2168. (In Japanese)
5) Fukuuchi Y, Teramoto J, Tatsuoka Y, Yamaguchi S, Watanabe Y, Shimizu T, Urashima N, Nishioka H, Iwasaki H: Clinical use experience of Imigran Kit Subcutaneous Injection 3 mg. Clinical evaluation of Imigran Kit Subcutaneous Injection 3 mg (sumatriptan succinate) for migraine and cluster headache. J Clin Therap Med 2008; 24(9): 809-824. (In Japanese)
6) Shimizu T, Sakai F, Tanaka R, Kato M, Ijiri S: Postmarketing surveillance of sumatriptan self-injection for migraine and cluster headache. J New Rem & Clin 2010; 59(5): 770-784. (In Japanese)
7) O’Quinn S, Davis RL, Gutterman DL, Pait GD, Fox AW: Prospective large-scale study of the tolerability of subcutaneous sumatriptan injection for acute treatment of migraine. Cephalalgia 1999; 19(4): 223-231.
8) Gobel H, Baar H, Beikfner HD, Bhme K, Beckmann-Reinhold A: Practicability and acceptance of subcutaneous self-administration of the selective serotonin agonist sumatriptan. Headache 1998; 38(4): 267-269.
9) Jensen K, Tfelt-Hansen P, Hansen EW, Kris EH, Pedersen OS: Introduction of a novel self-injector for sumatriptan. A controlled clinical trial in general practice. Cephalalgia 1995; 15(5): 423-429.
10) Gross ML, Kay J, Turner AM, Hallett K, Cleal AL, Hassani H: Sumatriptan in acute migraine using a novel cartridge system self-injector. United Kingdom Study Group. Headache 1994; 34(10): 559-563.
• Search terms and secondary sources
• Search database: PubMed (2011/12/22)
Sumatriptan
& ({subcutaneous} OR {injection} OR {self-}) 549
84 articles adopted from screening title and abstract
6 articles adopted after reviewing abstract and text
• Search database: Ichushi Web for articles published in Japan (2011/12/22)
Sumatriptan & injection 127
16 articles adopted from screening title and abstract
3 articles adopted after reviewing abstract and text